Meralgia Paraesthetica (MP) is an unusual condition that is characterized by a burning pain and sensory abnormalities (tingling and/or numbness) affecting the outer side of the thigh.
It is caused by pressure on/compression of a nerve – the lateral cutaneous nerve of the thigh (LCNT)(also known as the lateral femoral cutaneous nerve) – as it crosses from the lower abdomen into the upper thigh. It travels through a small tunnel on the outer aspect of the inguinal ligament – a fibrous band structure that runs from the bump at the front of the pelvis above the hip (the anterior superior iliac spine) to the inner part of the groin (pubic bone). Meralgia paraesthetica is classically caused when the LCNT is squashed as it travels through this tunnel. As this nerve is a sensory nerve only – compression causes pain and sensation disturbance but doesn’t cause any muscle weakness/paralysis.
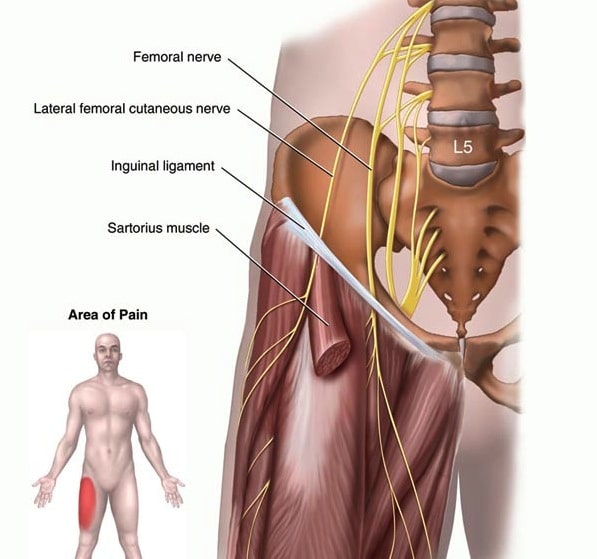
Figure 1. Meralgia Paraesthetica – Entrapment of the Lateral Femoral Cutaneous Nerve as it passes under the Inguinal Ligament.
Meralgia paraesthetica classically occurs in middle age (40-60 years) and in both males and females. In most cases there is no identifiable cause of this condition but there are definite associations with obesity and diabetes. Direct pressure on the front of the pelvis from tight clothing (jeans and belts), seat belts in cars, tool belts and pregnancy can be implicated at times.
The main symptom in MP is burning pain over the outer aspect of the thigh, along the line of the LCNT. This is usually constant and doesn’t change with rest or activity but may be aggravated by direct pressure over the front of the pelvis.
There may be sensitivity of the skin of the thigh to light touch and sometimes tapping over the course of the nerve where it crosses the inguinal ligament can produce pain and tingling in the thigh.
MP is largely a clinical diagnosis – there are no definitive tests for this condition, although nerve conduction studies can be helpful if positive.
Treatment in the first instance usually involves an injection of local anaesthetic and cortisone delivered around the nerve as it runs through the inguinal ligament. This is generally best done by a radiologist using ultrasound to localize the nerve. This injection can be helpful in confirming the diagnosis if it eliminates the pain of MP in the first few hours whilst the local anaesthetic is working. In many patients a single injection is all that is required but sometimes its effect wears off after resolution of symptoms for weeks or months. It can be repeated if helpful initially for a reasonable period. Weight reduction, optimal control of diabetes and attention to tight clothing and seat belts etc. should be addressed if appropriate.
Surgical decompression of the nerve may be indicated in cases unresponsive or recurrent with conservative treatment. Surgery involves dividing the tissue of the roof of the tunnel, releasing pressure on the nerve as it travels through the inguinal ligament. In cases where the condition has been present for a long time, surgical decompression of the LCNT may not relieve the condition completely and numbness/tingling may persist.
Source: https://www.parkclinic.com.au/meralgia-paraesthetica/