Total Hip Replacement (THR) is a surgical procedure that is arguably the most effective in all of medicine. In the right individual it can dramatically change a persons life providing improvements in pain relief and quality of life in a very cost effective way. 34,000 hip replacements were performed in Australia in 2010 and this number is increasing slowly each year.
Indications for Total Hip Replacement
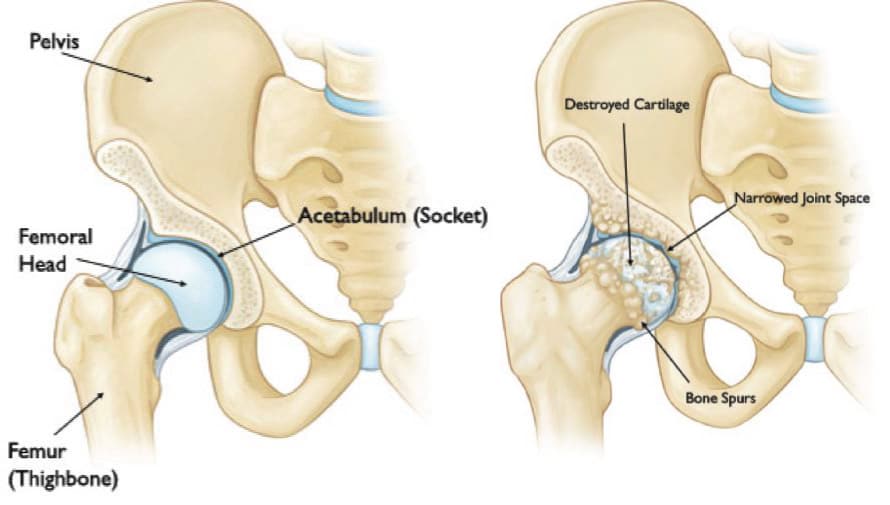
THR is potentially indicated when the normal surfaces of a hip joint have been damaged irretrievably. The common causes for this are:
- Osteoarthritis – a degenerative “wear and tear” condition seen generally in adults over the age of 50 years. The cartilage cushioning layer on the surface of the ball and socket of the hip wear away leaving “bone on bone” contact causing pain and stiffness.
- Inflammatory Arthritis (eg Rheumatoid Arthritis) – an auto-immune disease where the synovial lining of the joint becomes chronically inflamed and the cartilage surfaces of the hip joint become progressively destroyed.
- Avascular Necrosis of the Hip – an unusual condition where the blood supply to the ball of the joint fails leading to collapse of the bone directly beneath the joint surface. This leads to destruction of the smooth joint surface of the ball.
- Fracture of the Hip – very occasionally the fracture is such that hip replacement is indicated.
These conditions cause hip girdle pain and stiffness. This generally affects all weight bearing activity including walking, standing and all manner of recreational activity, rising from a seated position and tasks that involve bending such as getting shoes and socks on and off. If conservative treatment in the form of medications, changes in everyday activities, weight reduction if appropriate and the use of walking aids do not help the pain and stiffness, then hip replacement may be appropriate. In these circumstances hip replacement can provide pain relief, increase in hip motion and allow a return to normal daily activities including some simple exercise/recreations. Hip replacement surgery however is generally last resort treatment in a patient who has severe symptoms, advanced “bone on bone” disease in whom there is little prospect of improvement.
What is Total Hip Replacement?
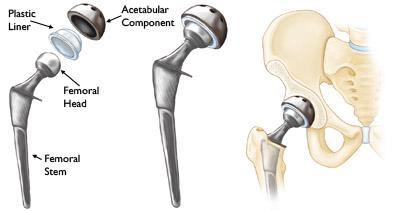
Conventional Total Hip Replacement involves replacing the worn surfaces of the hip joint with an artificial socket and ball. The new socket or acetabular component can be one piece but nowadays is most commonly a two piece device – consisting of a metal hemispherical shell and a separate bearing liner that can be made of a number of different materials. On the ball side of the joint (the femoral component) usually a stem is implanted into the central cavity of the upper femur and a ball is impacted onto the end of this stem. The ball itself can also be made of different materials and come in different sizes, allowing a “best” match or fit for each individual. Resurfacing Total Hip Replacement is a different type of THR, which involves insertion of a one-piece socket and a metal cap is placed over the ball. This technique has a limited place in the management of osteoarthritis.
THR components – acetabular (socket) and femoral stems – can be either cemented into place using an acrylic cement to anchor the component to the bone OR uncemented using a special surface on the component to get the bone of the socket or femur to grow onto the surface and lock them in place. Most acetabular components used nowadays are uncemented and rely on the coarse honeycomb like bone of the natural socket to grow into the gaps on a roughened or meshed surface on the back of the implant, effectively locking it in place. Sometimes in diseased or fragile bone using cement is better. The bone of the cavity or canal of the upper femur is much more solid, like a pipe – in this circumstance an uncemented femoral stem can be implanted tightly against this bone or an acrylic cement can be used to secure the implant. There are pros and cons to each approach.

Figure 4. An example of an uncemented femoral component with porous coated surface (arrows).

Figure 5. An uncemented acetabular component (socket) with polyethylene liner (left) and backside porous coating (right).
THR components can be made of different materials – non-corrosive metal alloys for the socket shells and femoral stems and polyethylene (a specialized “plastic” known as UHMWPE), ceramic or polished metal for the bearing surfaces of the ball and socket liner. Again there are pros and cons as to the constituents of the bearing surfaces in particular. There are a number of different models of hip replacement – a bit like different models of cars. They all have significant similarities with slight design or “accessory” differences but generally there is no one brand or type of prosthesis that is superior. Your surgeon will generally decide which would be the best for each individual and if you have questions regarding these issues just ask your surgeon.
Once a decision has been made to proceed with THR surgery, it is important that both parties involved – the patient and the doctor – work together to achieve the best result possible. Probably the most important issue in this regard is having a realistic expectation about what the outcome can be after surgery. Unfortunately THR is not a perfect technology and it can never give the recipient a “normal” hip.
Expectations with Total Hip Replacement
As such THR is a compromise operation – a compromise between a very arthritic hip and a normal hip. Our hope as surgeons is that a replaced hip would be very much at the normal end of the scale but the result can vary a little from person to person. A reasonable expectation would be a significant improvement in pain control particularly and hopefully a commensurate improvement in ability to undertake activity. Improvements in hip motion are variable but THR will not restore full motion. Most individuals are able to walk good distances unaided but occasionally gait aids/sticks are required – often to assist with balance and safety. Recreational pursuits such as swimming, cycling, gentle gym and exercise classes and bowls or golf can be undertaken. It is not advisable to undertake high impact activity such as running or jumping/jarring sports as this has the potential to prematurely wear out the bearing surfaces of any hip replacement. It is difficult to predict how long a replacement will last before it wears out requiring further surgery. This clearly depends on a number of factors but our best guess at this stage is that most modern THRs will probably last somewhere between 15 and 20 years. Unfortunately some hips fail earlier than this time frame. Putting things bluntly – you may need another operation to re-do or revise your THR if …… it wears out before you wear out!
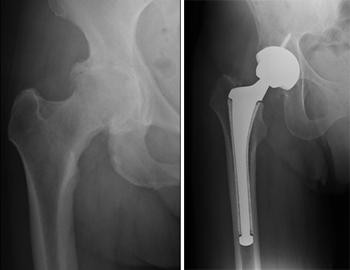
Figure 6. Xray of an arthritic hip before (left) and after total hip replacement (right).
The Procedure
The surgery itself takes approximately 2 hours to perform. Anaesthesia is required and can be a general or a regional anaesthetic or a combination of these two types. The anaesthetist will come and see you before surgery to discuss the type of anaesthetic that will be the safest for you – again there are pluses and minuses to each anaesthetic. Your surgeon will see you before your anaesthetic to answer any questions and most importantly to mark the surgical side/site with an indelible marking pen.
THR can be performed by a number of different approaches – this dictates which tissues/muscles are opened on the way to accessing the hip joint. The approach undertaken dictates where the skin incision is performed. Different approaches to the hip joint include the posterior approach, lateral approaches and an anterior approach. Again each approach has advantages and disadvantages. Successful THR can be performed through any of these approaches. Should you have any questions regarding approach, talk to your surgeon. Once the selected implants have been inserted the wound is closed with stitches or surgical clips and a dressing is applied. One or two drain tubes are left in the wound to drain any blood that may collect in the area. A special pillow is usually placed under or between the legs and this retained for the first few days post operatively.

Figure 7. A Gutter Pillow. This pillow is used under the operated leg in the early post operative period.
Post Operation and Recovery after Total Hip Replacement
Most patients undergoing THR surgery will stay in hospital around 5 days and in some cases a further stay for rehab is advisable. Your surgeon, supervising physiotherapist and nursing staff will advise you in this regard and make any arrangements that are necessary. Generally the day after surgery is a quiet day but usually involves a regime of bed exercises, standing out of bed with the physio and undertaking some limited walking. A blood test to check blood/haemoglobin levels and an xray of the new hip is usually performed. The drains are usually removed at the start of the second day and proper walking and standing exercises are begun. Over the next few days a progressive mobilization program with crutches is instituted with the aim of achieving readiness for discharge home. You need to able to walk a reasonable distance, dress and shower and negotiate stairs safely before going home. You need to understand that there are safe and unsafe ways of undertaking bending and rising tasks – your physio will teach you the correct way to do things.
Once at home it is recommended that you sleep on your back with a simple pillow between your legs in the first 6 weeks. You will generally need to use crutches and wear some compression or anti-embolic stockings in the first 6 weeks. At 12-14 days post surgery an arrangement will be made for a nurse to visit to remove any skin stitches or clips. At home you need to continue the mobilization program started in hospital with walking and gentle strengthening exercises. Driving is generally not advised in the first 6 weeks. At the 6 week mark a post-operative appointment with your surgeon is made to check your progress, answer any questions and to view some up to date xrays. All being well you can come off crutches and increase activity as comfort and confidence will allow. Your surgeon will talk to you about some simple “hip precautions” to safe guard your hip against problems. Most individuals having hip replacement will take 6 – 12 months to properly get over the surgery and back into normal levels of activity again.
Risks and Potential Complications
There are some risks associated with THR surgery, just as there are with any surgical procedures. These risks can be broken down into general risks (that exist with any reasonable sized operation) and specific risks that relate to Total Hip Replacement itself. The risks listed below are the most common issues but this list is by no means all inclusive – if you have any concerns about these or any other risks, talk to your surgeon before surgery.
General risks include:
- Anaesthesia – modern anaesthesia is very safe, but with whichever method of anaesthesia is undertaken, there are very small risks. If you concerns in this regard, please talk to your anaesthetist when he/she comes to see you before surgery.
- Medical complications – chest and urinary infections, blood pressure and cardiac/other issues can occur following any significant surgery.
- Infection – there is approximately a 1% chance you could develop a significant infection in your hip. Antibiotics given at the time of surgery and post-operatively reduce this risk but do NOT entirely negate it.
- Deep Vein Thrombosis – this is a clot that can occur in the deep veins of the leg, usually beginning in the calf. Again this risk is minimized by medication, anti clot stockings and early mobilization but none of these things guarantees prevention. If serious, the clot could travel to the lung and in very rare instances this can be fatal. If you have had a thrombosis in the past, you are at greater risk of this complication – let your surgeon know if this is the case.
- Blood Loss – THR surgery is associated with some blood loss and occasionally a blood transfusion is required.
- Nerve or Vessel Damage – there are large vessels and nerves that travel into the leg both in front of and behind the hip. Damage to these structures is rare but possible.
Specific risks include:
- Dislocation – the ball and socket arrangement of a hip replacement is not as stable as a natural hip and sometimes can dislocate. The risky period is the first 6-8 weeks and it is over this time that strict hip precautions are in place. You will be advised of dangerous positions for your hip whilst in hospital. Dislocation can occur after this period but usually relates awkward movements when attempting bending/reaching tasks particularly when the hip is in a very flexed position.
Figure 8. Dislocation after Total Hip Replacement – the femoral head (ball) has completely come out of the acetabulum (socket).
- Leg Length – sometimes, hip replacement will alter the length of the leg being operated on. The aim of THR surgery is to leave both legs the same length but sometimes this is not possible for various reasons. Most discrepancies in leg length are small and not noticeable. Very occasionally the discrepancy can be larger and if this is the case insoles or shoe raises for the affected leg may be required to feel balanced when walking or standing.
- Implant Wear and Loosening – the bearing surfaces of a hip replacement will slowly wear down over time. As stated previously, it is hoped that these surfaces will last 15 – 20 years and sometimes beyond. There is always a possibility that a hip replacement may wear out or loosen at any stage even early, requiring further surgery.
As stated above this list of risks and potential complications is not exhaustive and if you have any concerns, please raise these with your surgeon before proceeding with hip replacement surgery.
Despite these potential issues, the outcome following THR surgery is in most cases excellent with markedly improved pain and function. Unfortunately, as with any operative procedure there is no surgery that is 100% successful and a small percentage of individuals may continue to have some pain and limitation.
Source: https://www.parkclinic.com.au/total-hip-replacement-surgery/