
Presentation
83yo retired lady presented with a complaint of a painless limp affecting the left leg. She first noticed this 10 years ago and felt that it was getting worse. This affected her ability to walk distances, her balance and she reported that she fatigued easily with any weight bearing exercise. Interestingly she felt her gait was better if she took quick, small steps. No history of any pain in the leg, around the hip or back. No lower limb paraesthesia. Undertaking hydrotherapy classes under the guidance of a physiotherapist. No history of diabetes. On non-statin medication for hyperlipidaemia.
Exam Findings
Lurching gait not antalgic. Trendelenburg test positive. 0.5 – 1 cm shortening of left leg. Left hip – no fixed contracture, good painfree range of movement. Neuro left leg – decreased power hip abduction, slightly reduced hip flexion power but all other muscle groups normal. Intact sensation. All reflexes difficult to elicit in both legs.
Investigations
MRI lumbar spine – mild multilevel disc degeneration without canal or foraminal stenosis. MRI left hip – complete tears of both gluteus medius and minimus tendons with retraction. Gluteal muscle atrophy with fatty infiltration. Minor degenerative articular changes in hip joint.

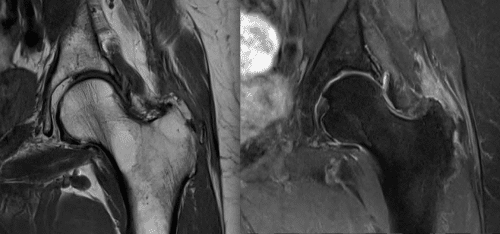
Figure 1. Left: MRI scan T1 image of normal hip with gluteus minimus tendon (*) and gluteus medius tendon (**). Middle: MRI T1 image of torn gluteus and minimus tendons. Note muscle belly atrophy. Right: Corresponding MRI T2 image.
Diagnosis
Limp caused by gluteal weakness secondary to chronic tear of main hip abductors – gluteus medius and minimus.
Differential Diagnosis
Causes of a unilateral Trendelenburg gait (pain, disruption of the lever arm or weakness). Weakness of gluteal musculature due to neurological deficit (superior gluteal nerve palsy, lumbar plexopathy, polio), local muscular problem (myopathy, muscular dystrophy) or intrinsic hip joint disorder (OA, Dysplasia, Fracture).
Recommendation
Conservative management with continuation of an exercise program for general strengthening and balance, insole left shoe to correct minor leg shortening and particularly the use of a stick in the right hand to assist with ambulation. Surgical repair was not contemplated.
Case Comment
An unusual case. Most Trendelenburg limps are associated with pain, due to hip arthritis or other local hip pathology.
Surgical repair of torn tendons in this circumstance would be highly unlikely to provide any benefit to the patient. The patient’s age would likely mean that tendons would be degenerate and tissue of poor quality. The duration of symptoms and absence of a history of significant injury indicates a chronic process. Retraction of the tendons means that repair would be technically difficult and likely to fail either at the repair site or in the tendon substance itself proximal to the repair. Fatty atrophy of the driving muscle unit indicates that even if a solid repair of good quality tendon tissue could be achieved, there would still be significant weakness of hip abduction essential for balance and walking endurance due to the small numbers of muscle fibres able to contract effectively. Surgery in this circumstance involves some risk to the patient (general risks and risk of complication like infection, deep vein thrombosis and nerve/vessel injury) and a prolonged recovery/rehab period with minimal chance of an outcome that would be significantly better than conservative management.
