I attended our regular journal club meeting for March 2016 where a number of interesting papers focusing on joint replacement and knee surgery were discussed.
The most intriguing paper of the evening was one looking at the old “chestnut” topic of computer navigated versus conventional Total Knee Replacement (TKR) – which is better? This study out of South Korea had a number of unique design features and importantly a disclosure statement indicating no conflict of interest (no relationships with and no funds received by any implant company) – quite unusual for a study of this size.
The study was a single surgeon series of an amazing 520 patients who each underwent bilateral total knee replacement (1040 knees studied) at a single institution. With each surgery one knee was randomly assigned to computer navigated knee replacement whilst the other underwent a conventional TKR procedure – a controlled trial of technique in each patient!
Interestingly 85% of the patients were female, with an average age of 68 years and an average BMI of 27 – a slightly different demographic to our standard Australian population undergoing TKR.
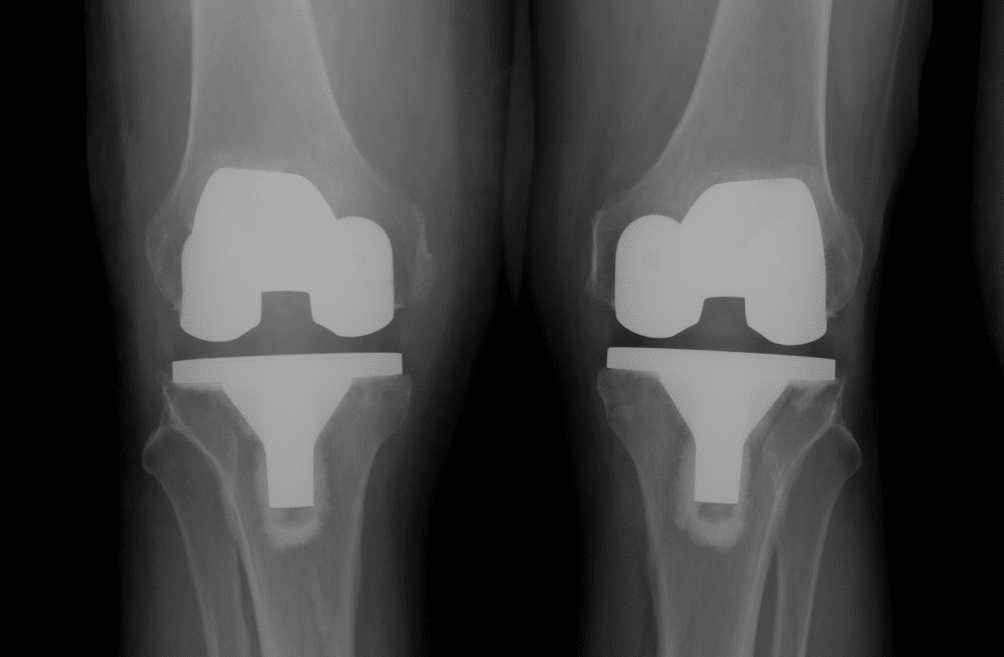
These patients were followed prospectively for an average of 10.8 years with clinical (Knee Society, WOMAC and UCLA activity scores), radiological (long leg alignment xrays and CT) assessment and survivorship analysis being undertaken.
A number of authors in the past have espoused the advantages of computer navigated over conventional TKR with regard to implant alignment and unrelated retrospective studies have suggested that an optimal “window” of alignment (3 degrees either side of neutral mechanical alignment) corresponds with better long term implant survivorship.
This paper indicated that in this quite unique cohort of patients, there was no difference in clinical scores for pain and function, no difference in implant alignment radiologically in either coronal and rotational planes and most importantly no difference in survivorship of implant between conventional technique and computer navigated TKR groups over a 10 year follow up period.
The strengths of this study were the large number of TKRs studied, the fact that all procedures were performed by a single surgeon (allowing reliability of technique) and most importantly some medium to long term follow up both clinically and radiologically. The weaknesses of the study were that interpretation of pain and function scores would not necessarily select out one knee group over another and this cohort of patients is demographically quite different to a Western society population undergoing TKR. It would have been really interesting (but not necessarily scientific) if patients were asked which knee they preferred or felt was better and to see if there was a difference between the groups.
Ultimately there is no best or superior way to undertake total knee replacement. Straightforward cases can be performed well by any experienced surgeon with conventional instrumentation and techniques. There are undoubtedly difficult cases, particularly those with significant bony deformity around the knee, where computer navigation or now patient specific instrumentation can be beneficial to both patient and surgeon.
Source: Computer-Navigated Versus Conventional Total Knee Arthroplasty. J Bone Joint Surg Am. 2012; 94: 2017-24.